About Living Well, Your Way
It all begins with an idea. Maybe you want to launch a business. Maybe you want to turn a hobby into something more. Or maybe you have a creative project to share with the world. Whatever it is, the way you tell your story online can make all the difference.
Collaborative Commissioning
Origin & development
Murrumbidgee Primary Health Network (MPHN) and Murrumbidgee Local Health District (MLHD) Collaborative Commissioning partnership was formed to develop and implement a care pathway for people living with Chronic Obstructive Pulmonary Disease (COPD) and/or Congestive Heart Failure (CHF). In 2019, the Patient Centred Co-Commissioning Governance (PCCG) group was established to oversee the development of the Living Well, Your Way initiative.
Living Well, Your Way (‘the Pathway’) has been created with the following guiding principles:
No step in the pathway is finished until the next has started.
Clinicians working to the top of their scope.
Collaboration between providers.
Alternatives to the emergency department.
Patient focused; Data driven.
Pathway Co-design
In 2019 co-design of LWYW began with significant consultation of a wide range of stakeholders from across the region. Virtual co-design events with 12 workshops were held over three days in October 2021, consulting with the equivalent to 200 people (noting that some individuals participated in more than one workshop).
Attendees included representatives from general practice, pharmacy, allied health, health consumers, Aboriginal health staff and community leaders, Ministry of Health, and MLHD and MPHN staff and Executive.
The following program was developed.
Pre-Development Phase
Aim: Assess the ways people with COPD and CHF receive care and support to manage their condition by asking lots of questions and reviewing lots of data.
This phase began in 2020 with the formation of the Collaborative Commissioning team and securing funding.
Joint Development Phase (Design and Costing)
Aim: Ask how patient health journey can be improved and design a new and better pathway of care.
In July 2021 consultation began with key stakeholders to clarify the target patient cohort and their qualifying criteria. The Collaborative Commissioning Team began mapping the new care pathway including costings and the summary of benefits for this cohort and services. This is where the Pathway was born.
Feasibility Phase
Aim: Put the new design to the test to see how well it serves everyone, especially the individuals living with COPD and CHF. Trial and adopt with as many patient volunteers as possible to ensure it is feasible and that the data and patient journey both improve.
The feasibility phase allowed trial of the models of care developed during consultation and assess their effectiveness and sustainability. The trials rolled out across selected communities, reviewed with the intention to expand over time.
Implementation Phase
Aim: Keep going and apply the same pathway to more people and other chronic conditions.
Vision
People living with CHF and/or COPD in our community – no matter where they live – should have the best quality of life possible by having access to the personal, professional, and community resources they need, when they need them, and in the way that they choose to use them.
Changing the way healthcare is accessed and delivered, may assist people to self-manage their chronic conditions effectively and sustainably, to live well at home and in the community reducing the need for avoidable hospital admissions.
The pathway enabled health professionals to focus on patient centred care, working together as a team, providing targeted collaborative values-based care.
LWYW Goals were:
To promote care in the community.
To enhance individual’s abilities to stay healthier at home for longer.
To create a local culture of collaboration.
To support the delivery of exceptional rural healthcare.
To improve the efficiency and effectiveness of healthcare delivery for people with chronic disease in the Murrumbidgee.
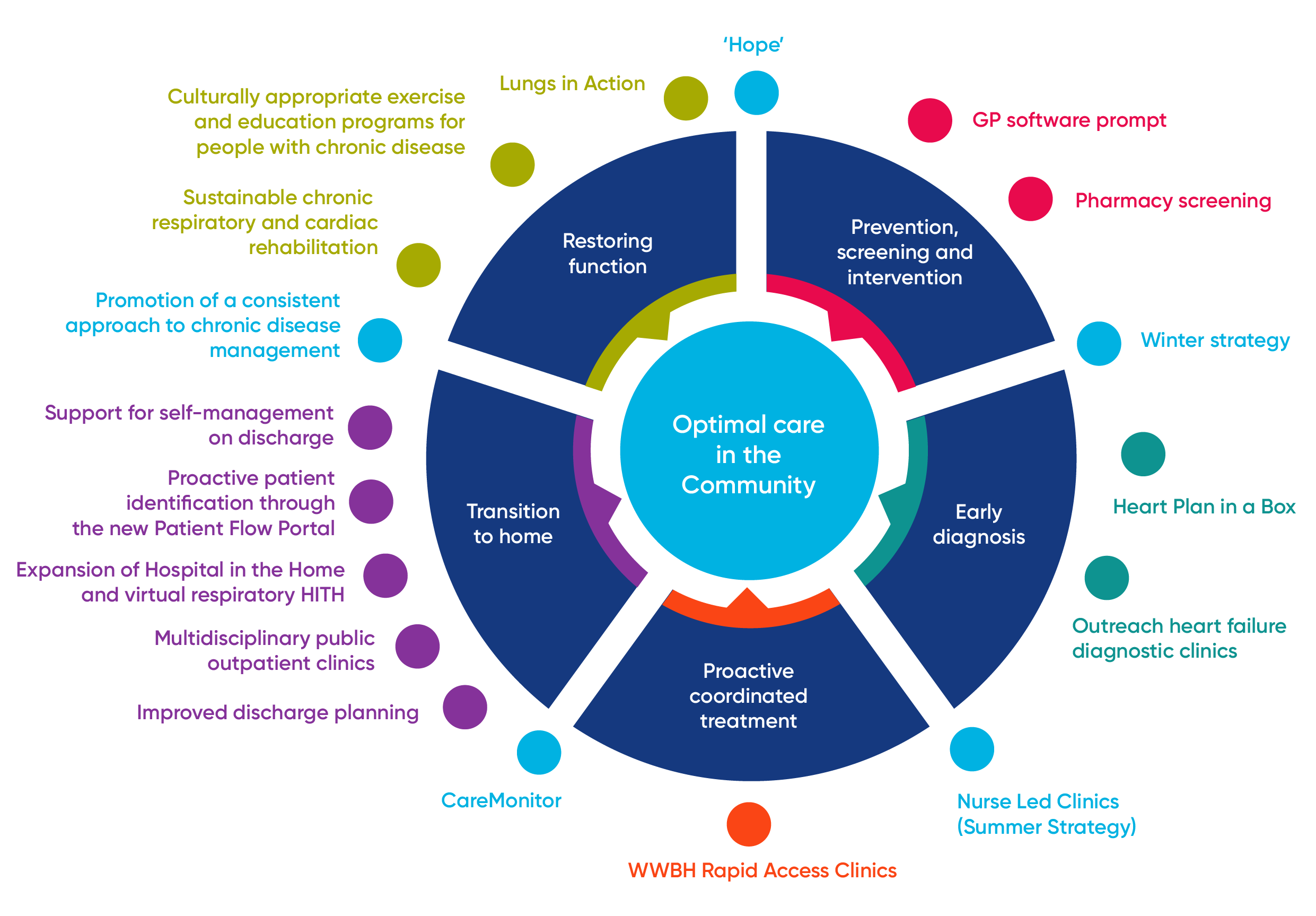
The Living Well, Your Way Pathway
Click on the magnifiers to see our partners and partnerships along The Pathway.
Objectives of the Pathway
The goal of the Pathway is to keep people with COPD and/or CHF healthier at home for longer. The targeted outcomes include:
Improved quality of life for people with COPD and CHF.
Reduced demand for hospital services for people with COPD and CHF.
Reduced avoidable mortality for people with COPD and CHF Overview of the Pathway.
Key principles underpinning the Pathway:
Consumers should always be in the community unless it is clinically unsafe to do so.
Each point of service is to ensure the consumer is linked to the next appropriate service so there is continuity through the Pathway.
An individual may enter the Pathway at any stage, however, the primary goal is for the individual to return to and remain in ‘optimal care in the community’.
The long-term aim is for every consumer to have one Health and Wellbeing Plan, which integrates existing action plans and care plans, and is ‘translated’ into non-clinical language and connected to the consumer’s personal circumstances.
The Pathway is comprised of seven key focus areas (stages) which encompass the whole of health care system in the Murrumbidgee region.
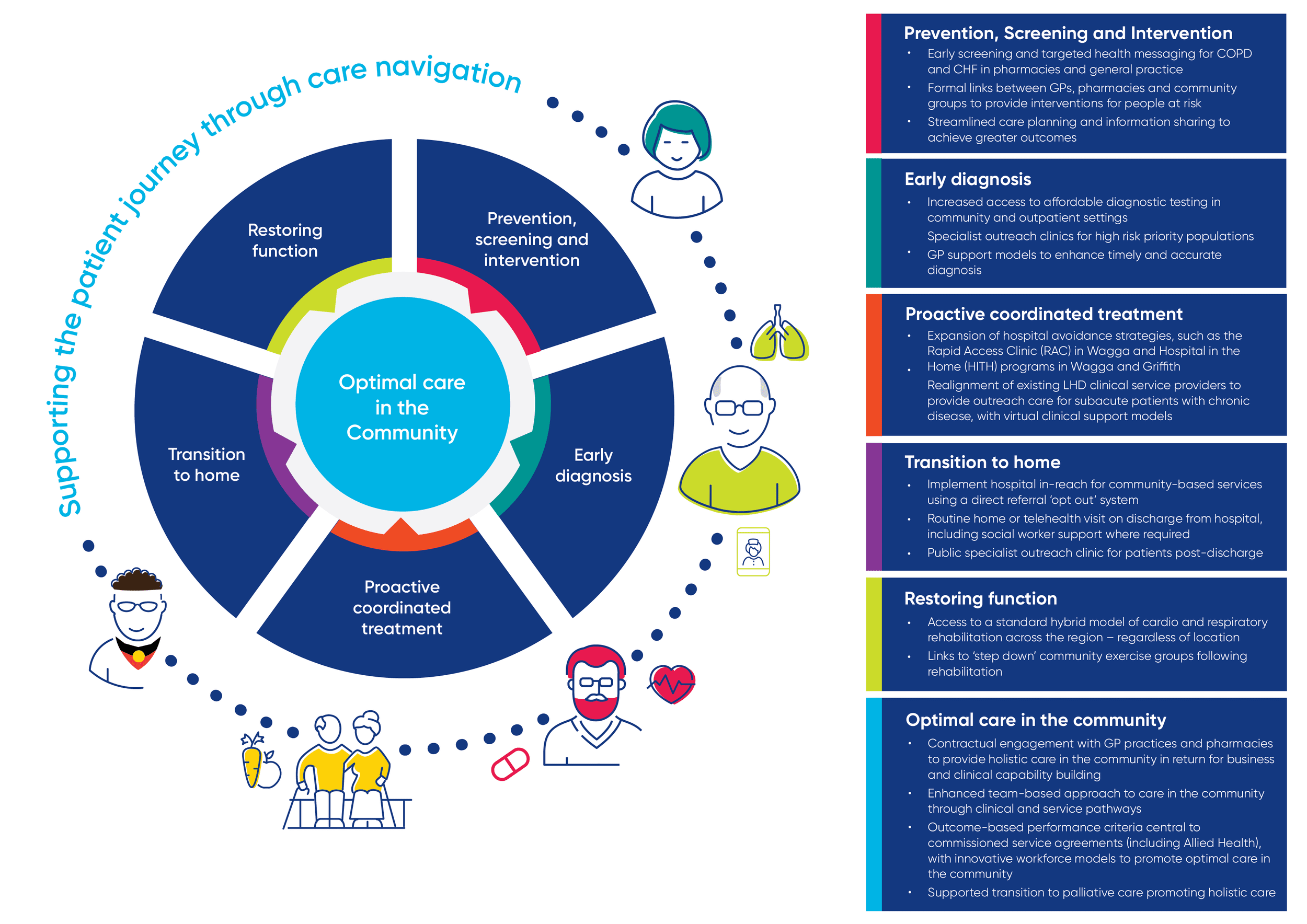
Prevention, Screening & Intervention
Early screening and targeting health messaging for COPD and CHF in pharmacies and general practice.
Formal links between GPs, pharmacies and community groups to provide interventions for people at risk.
Streamlining care planning and information sharing to achieve greater outcomes.
Early Diagnosis
Increased access to affordable diagnostic testing in community and outpatient settings.
Specialist outreach clinics for high risk priority populations
GP support models to enhance timely and accurate diagnosis.
Proactive Treatment
Expansion of hospital avoidance strategies such as the Rapid Access Clinic (RAC) in Wagga and Hospital in the Home (HITH) Programs in Griffith and Wagga.
Realignment of existing LHD clinical service providers to provide outreach care for subacute patients with chronic disease, with virtual clinical support models.
Transition to Home
Implement hospital in-reach for community-based services using a direct referral ‘opt-out’ system.
Routine home or telehealth visit on discharge from hospital including social worker support where required.
Public specialist outreach clinic for patients post-discharge.
Restoring Function
Access to a standard hybrid model of cardiorespiratory rehabilitation across the region – regardless of location.
Links to step down community exercise groups following rehabilitation.
Optimal Care in the Community
Contractual engagement with GP practices and pharmacies to provide wholistic care in the community in return for business and clinical capacity building
Enhanced team-based approach to care in the community through clinical and service pathways.
Outcome-based performance criteria central to commissioned service agreements (inc allied health) with innovative workforce models to promote optimal care in the community.
Supported transition to palliative care promoting holistic care.
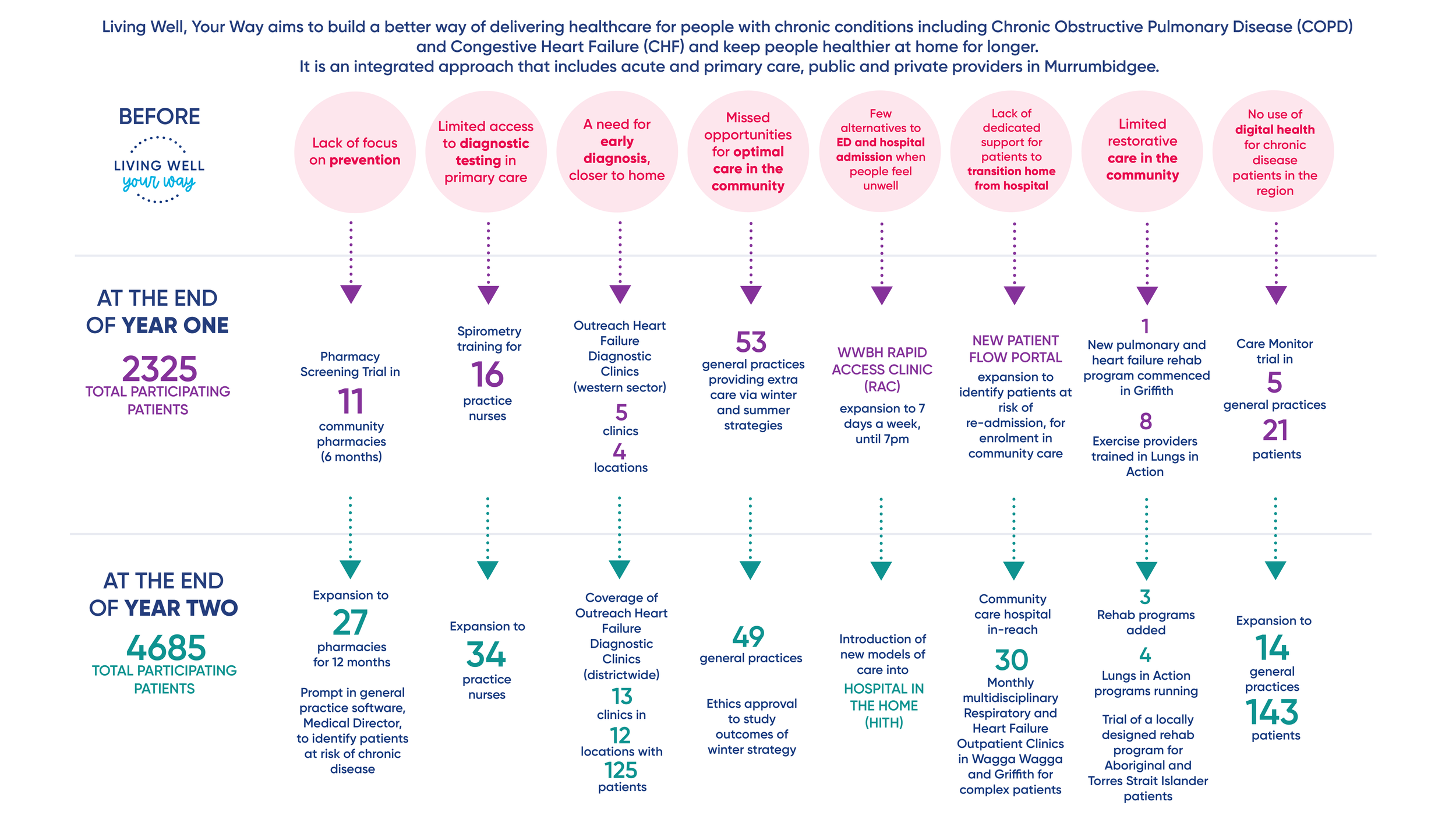
Our activities
Results